Saturday, February 18, 2006
New training session in Valencia
Last friday I travelled to Valencia to participate in a training session that would entail operating four patients. On friday I performed a Greenlight PV procedure on a patient with a 90 g prostate. Then I was taken for dinner to a very nice vasc restaurant. After a short sleep (we had dinner at 11.00 pm) we started early on Saturday morning and I operated three more patients with a 60 g prostate, then a 90 g prostate and then the last patient's prostate weighed 130 g. We finished at 5.00 pm and then I returned to Madrid, totally exhausted after a very intense week.
Friday, February 17, 2006
Training Session in Robotic Surgery
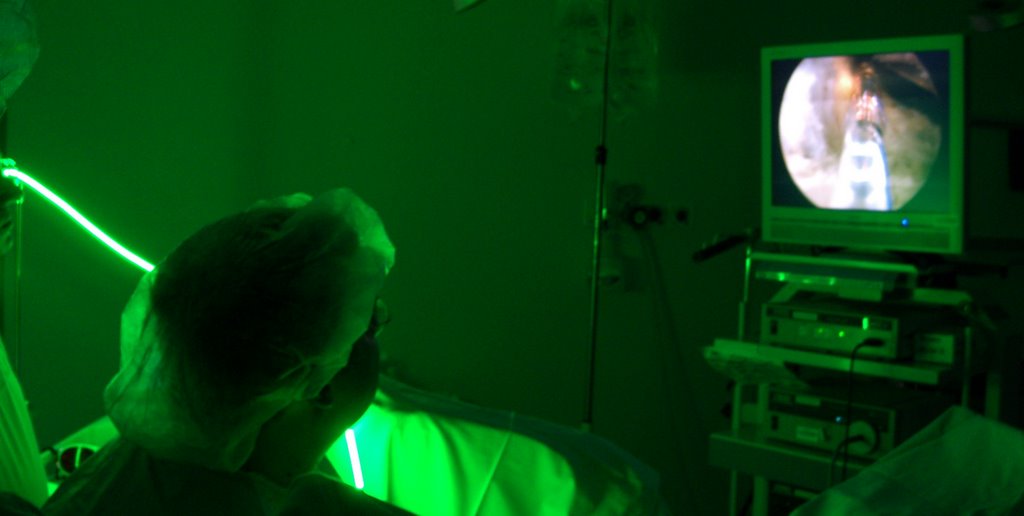
 Today I took a plane with my colleague, Dr. Castillón to participate in a training session on Robotic Radical Prostatectomy with the Da Vinci system. This system allows the surgeon to operate from a surgical station, as in the photograph, and provides 3D visualization of the operative field inside the abdomen. This is the state of the art treatment for localised prostate cancer and it allows to obtain spectacular oncological results, as well as high rates of urinary continence and sexual potency preservation after this operation, that are not obtainable with open surgery.
Today I took a plane with my colleague, Dr. Castillón to participate in a training session on Robotic Radical Prostatectomy with the Da Vinci system. This system allows the surgeon to operate from a surgical station, as in the photograph, and provides 3D visualization of the operative field inside the abdomen. This is the state of the art treatment for localised prostate cancer and it allows to obtain spectacular oncological results, as well as high rates of urinary continence and sexual potency preservation after this operation, that are not obtainable with open surgery.We are trying to achieve to adopt this technology at the Instituto de Cirugía Urológica Avanzada, in collaboration with Hospital USP San José from Madrid. The problem is the high cost of this equipment, so if there is any benefactor reading this and wanting to help us, we will be happy to hear from him. We want to be able to offer this treatment for prostate cancer patients in Madrid. We are starting our training in order to be able to operate our patients soon.
This robot is intuitive and allows the surgeon to conduct surgical operations with safety and precision from the very beginning.
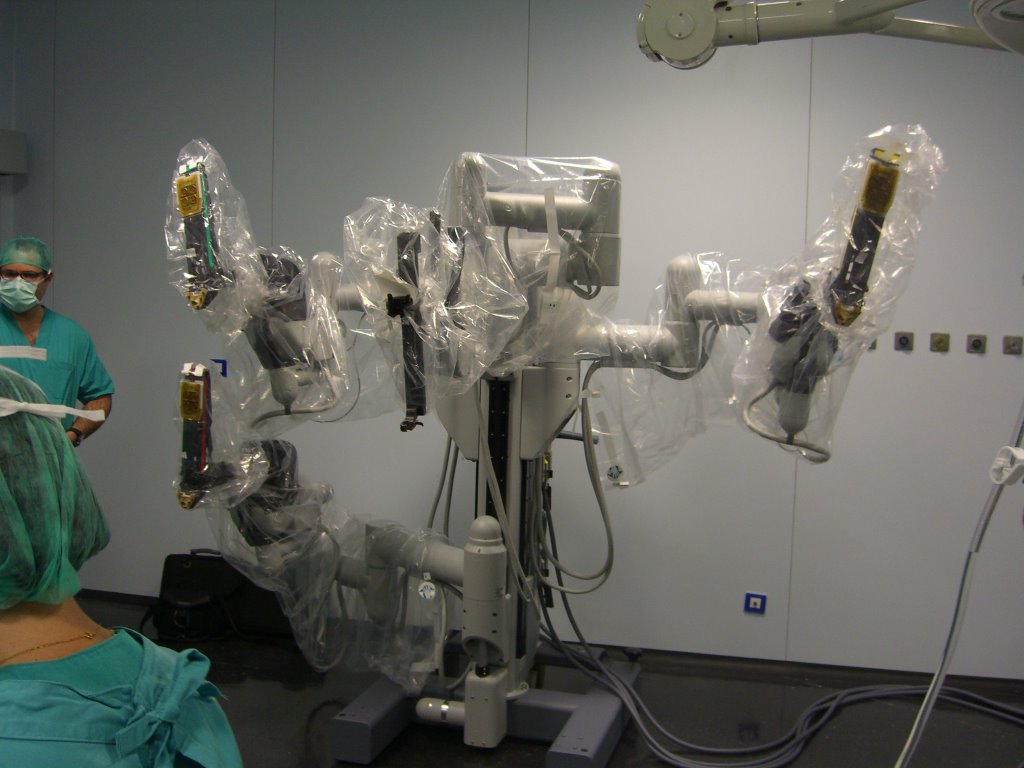 This is the robot and the four arms, it will be position by the patient and the robot will manipulate the surgical instruments. It is a slave robot, it obeys the movements of the surgeon hands, that holds two very sophisticated Joysticks with his hands. The robot even corrects tremor of the surgeon's hands. 3D vision inside the abdomen helps visualizing tissues with unseen quality of image and enhancement.
This is the robot and the four arms, it will be position by the patient and the robot will manipulate the surgical instruments. It is a slave robot, it obeys the movements of the surgeon hands, that holds two very sophisticated Joysticks with his hands. The robot even corrects tremor of the surgeon's hands. 3D vision inside the abdomen helps visualizing tissues with unseen quality of image and enhancement. The surgeon is relaxed, sitting in the surgical console, and an assistant changes the instruments of the robot when the surgeon requests it. It is no doubt the way surgery will follow in the future.
The surgeon is relaxed, sitting in the surgical console, and an assistant changes the instruments of the robot when the surgeon requests it. It is no doubt the way surgery will follow in the future.It is a fact, medicine is becoming more and more technologic, and technology is expensive. The best doctors in the future will not necessarily be those who study more, or those with more natural ability and dexterity for surgery, but those who have access to the latest technology, that will be very costly, but that will offer unparalelled results in the treatment of urologic diseases.
Monday, February 13, 2006
New training session in La Coruña
 Once again I flew to La Coruña to participate in a training session. In this ocassion we had a difficult case, a patient with a 135 gram prostate. After spending the afternoon there, I took the plane back to Madrid. This is a busy week, this Thursday I will do an early morning PVP and then I will take the plane to Bilbao, in the north of Spain. I am going to witness a case of radical
Once again I flew to La Coruña to participate in a training session. In this ocassion we had a difficult case, a patient with a 135 gram prostate. After spending the afternoon there, I took the plane back to Madrid. This is a busy week, this Thursday I will do an early morning PVP and then I will take the plane to Bilbao, in the north of Spain. I am going to witness a case of radicalprostatectomy for prostate cancer with the "Da Vinci" surgical robot. Then I will travel to Valencia Friday and Saturday, where I will conduct a training session where we will operate four patients. In order to make this posting more interesting, I will explain what kind of instruments we use for Greenlight PVP.
This is a photograph of the cystoscope we use for PVP, it is thinner than the classic resectoscope used in TURP (Transurethral resection of the prostate). The laser fiber is introduced throuhg the cystoscope's working channel, and is provided with a plastic knob that allows to rotate it, introduce it or withdraw it easily to ensure prostate vaporization.
 The black piece is the telescope's visor, traditionally one would look through it with the naked eye, but when working with lasers eye protection is a must, that is why we connect this visor to a surgical endoscopic video camera, but in order to protect the camera from the intensity of the greenlight laser (the reflection of the laser light could break the camera), we use a filter between the visor and the camera. This explains why in the photographs of the technique I publish here, the laser fibre appears green, but in the endoscopic videos the laser light looks like orange. This filter blocks the specific wavelenght of the greenlight laser (532 nm).
The black piece is the telescope's visor, traditionally one would look through it with the naked eye, but when working with lasers eye protection is a must, that is why we connect this visor to a surgical endoscopic video camera, but in order to protect the camera from the intensity of the greenlight laser (the reflection of the laser light could break the camera), we use a filter between the visor and the camera. This explains why in the photographs of the technique I publish here, the laser fibre appears green, but in the endoscopic videos the laser light looks like orange. This filter blocks the specific wavelenght of the greenlight laser (532 nm).
Thursday, February 09, 2006
Invitation to South Africa.
 Yesterday I received confirmation of an invitation to travel to South Africa to participate in lectures in different cities on Greenlight PVP (Photoselective Vaporization of the Prostate).
Yesterday I received confirmation of an invitation to travel to South Africa to participate in lectures in different cities on Greenlight PVP (Photoselective Vaporization of the Prostate).I was told that there are still no Greenlight units installed in South Africa, but there is a great interest in the technique.
After the workshop at King's Hospital in London I will depart to South Africa to participate in lectures in different cities in South Africa. I will return the 1st of April to Madrid.
I will update this entry as soon as I receive additional information.
Invitation to King's College Hospital, London
At last we have a definitive date for the meeting at Kings College Hospital in London. March 24th. Mr Gordon Muir is organizing a fantastic workshop devoted to PVP (Photoselective Vaporization of the Prosate). Lectures, round tables and live surgeries will take place in front of Urologists, GPs, anaesthetists and other people interested in this technique. I will contribute with a couple of presentations. I guess if someone wants to attend he will have to contact Mr. Gordon Muir at King's College Hospital, London.

New trip to India
Again I have been invited to travel to India. This time I will visit Hospital Prince Ali Khan in Mumbai. The first weekend of March I will spend some time there with the urologists to contribute to their training on PVP (Photoselective Vaporization of the Prostate).
Live surgery at the International Congress in Zaragoza
 Today I have participated in the Urology International Congress celebrated at the Hospital Miguel Servet, from Zaragoza, organised by profs. Rioja, Liédana y Roncales. It is a very impressive congress, the organization was superb and the scientific program very attractive. Multiple national and international experts were invited. The conference hall had three giant screens where urologists attending the congress could see three simultaneous surgical interventions and hear one of the three conversations going on between the surgeons and the moderators of each surgical session. Congratulations to the organisers!!!.
Today I have participated in the Urology International Congress celebrated at the Hospital Miguel Servet, from Zaragoza, organised by profs. Rioja, Liédana y Roncales. It is a very impressive congress, the organization was superb and the scientific program very attractive. Multiple national and international experts were invited. The conference hall had three giant screens where urologists attending the congress could see three simultaneous surgical interventions and hear one of the three conversations going on between the surgeons and the moderators of each surgical session. Congratulations to the organisers!!!.
 This Hospital Miguel Servet is interestingly in front of the football stadium "La Rosaleda", where the local team scored 6 goals to Real Madrid football club, who could one produce one miserable goal. I have had the strange feeling that everybody here looked suspiciously happy and their smiles were probably wider than usual. I am not exactly a football fan, but one perceives these things..... and my team is Real Madrid.
This Hospital Miguel Servet is interestingly in front of the football stadium "La Rosaleda", where the local team scored 6 goals to Real Madrid football club, who could one produce one miserable goal. I have had the strange feeling that everybody here looked suspiciously happy and their smiles were probably wider than usual. I am not exactly a football fan, but one perceives these things..... and my team is Real Madrid.My contribution to this scientific meeting was to perform a live PVP (Photoselective Vaporization of the Prostate). The patient was relatively young, and suffered Benign Prostatic Hyperplasia, and although the prostate was small, weighing 44 g, it caused him bothersome symptoms. After visiting him in the Hospital room and chatting for some time explaining the operation and what to expect in the postoperative period, I went down to the surgical theatre. They were operating another BPH patient with a monopolar electrosurgical unit. Monopolar resection is a sophistication of the instrument used for the classic transurethral resection of the prostate (TURP) it allows better cutting and apparently a shorter catheterisation time for patients. It uses saline as irrigant, and this avoids the TURP syndrom (absoption of irrigant into the bloodstream, and dylutional hyponatremia) that can happen when a solution with glycine is used as irrigant. But coagulation is less than perfect, and the patient bleeds during surgery. When they finished, a catheter was inserted and a traction was devised to diminish postoperative blood loss, they said the catheter would stay in for a couple of days.
 Then it was my turn. The PVP operation was uneventful and I was able to vaporise BPH tissue and reach the capsule of the prostate in just 45 minutes. During the operation, I had a microphone that allowed me to explain the operation and I also had an interesting conversation with the moderator, Dr. Miñana, who posed very interesting questions. I tried to summarize the advantages of this technique as well as the mechanisms of laser and tissue interactions. The audience was very impressed, specially after having seen a monopolar resection, which did not avoid bleeding.
Then it was my turn. The PVP operation was uneventful and I was able to vaporise BPH tissue and reach the capsule of the prostate in just 45 minutes. During the operation, I had a microphone that allowed me to explain the operation and I also had an interesting conversation with the moderator, Dr. Miñana, who posed very interesting questions. I tried to summarize the advantages of this technique as well as the mechanisms of laser and tissue interactions. The audience was very impressed, specially after having seen a monopolar resection, which did not avoid bleeding.The patient did not bleed at all, and he told me he was happy when he was being carried to the ward, as he had heard all my explanations during surgery. I asked the urologists who will do the follow up to pull his catheter out six hours after surgery and told them that he could be sent home later that day if they wanted. Each time I do this operation I get more convinced that PVP is superior to any kind of prostatic resection, be it with a bipolar or a monopolar generator.
After the succesful surgical session, I went to a local restaurant and then took the AVE (the high speed train) towards Madrid hoping to get some rest tonight.
Wednesday, February 08, 2006
New training session in TEKNON, Barcelona
 Today I travelled to Barcelona to participate in a training session on PVP (Photoselective Vaporization of the Prostate) for BPH (Benign Prostatic Hyperplasia). We did two cases, one was a very high risk patient, who was obese, and had an aortic aneurism, dilated myocardiopathy and other serious conditions. His prostate was relatively big, with 90 grams. The operation was uneventful and today we managed to finally operate him, as this time he did not take biscuits just before scheduled surgery (some days ago we had to cancel the operation for this reason). In spite of the high surgical risk, we managed to operate him and to let him catheter-free. He had been catheterised due to an acute retention of urine and after that, he was unable to void spontaneously. Then we did an easier case, a 60 g prostate, that was also uneventful. I then took a car and drove towards Zaragoza, a three hour trip to reach this city. Tomorrow I have to participate in the International Congress performing a live PVP in front of 200 + urologists from Spain and other countries.
Today I travelled to Barcelona to participate in a training session on PVP (Photoselective Vaporization of the Prostate) for BPH (Benign Prostatic Hyperplasia). We did two cases, one was a very high risk patient, who was obese, and had an aortic aneurism, dilated myocardiopathy and other serious conditions. His prostate was relatively big, with 90 grams. The operation was uneventful and today we managed to finally operate him, as this time he did not take biscuits just before scheduled surgery (some days ago we had to cancel the operation for this reason). In spite of the high surgical risk, we managed to operate him and to let him catheter-free. He had been catheterised due to an acute retention of urine and after that, he was unable to void spontaneously. Then we did an easier case, a 60 g prostate, that was also uneventful. I then took a car and drove towards Zaragoza, a three hour trip to reach this city. Tomorrow I have to participate in the International Congress performing a live PVP in front of 200 + urologists from Spain and other countries.
Sunday, February 05, 2006
Training session in Madrid
I operated three PVP patients this morning, all sufferers of Benign Prostatic Hyperplasia, and we had two visitors that came to the surgical theatre to see the operations. One was Dr. Camille Mugnier, from Bordeaux, France. He is Dr. Gastón's partner and he specialises in BPH. He was interested in PVP and after this session he was convinced to buy a Greenlight laser. The second visiting urologist was Dr. Virgilio Baz, from Lisbon, Portugal. He has already bougth it, and he wanted to see some procedures before starting offering this treatment to his patients.
We started with a 60 gram prostate, then a 30 gram prostate and finally, a relatively big 100 g prostate. Many urologists are skeptic about the fact that big prostates can be operated succesfully with PVP. ¿Is it possible to apply PVP to big prostates?
The answer is yes, but it is not an easy operation. The surgeon must be very experienced, he must have an "agressive" mentality, and try to vaporize as much tissue as possible, and he must be ready to spend as much time as necessary and as many fibres as needed. In this case, a 100 gram prostate, I used 430.000 joules with three fibres (they are more effective in their first 150.000 joules) in two hours. I operated this patient under spinal anaesthetic starting at 4.00 pm and he was discharged the following morning.
This is the ultrasound scan I took 30 hours after the operation. A central cavity is seen, similar to those seen after open prostatectomy.
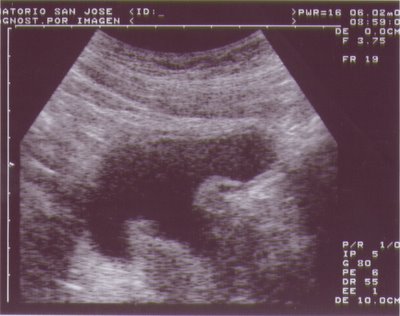
I would appreciate comments from visitors to this blog.
We started with a 60 gram prostate, then a 30 gram prostate and finally, a relatively big 100 g prostate. Many urologists are skeptic about the fact that big prostates can be operated succesfully with PVP. ¿Is it possible to apply PVP to big prostates?
The answer is yes, but it is not an easy operation. The surgeon must be very experienced, he must have an "agressive" mentality, and try to vaporize as much tissue as possible, and he must be ready to spend as much time as necessary and as many fibres as needed. In this case, a 100 gram prostate, I used 430.000 joules with three fibres (they are more effective in their first 150.000 joules) in two hours. I operated this patient under spinal anaesthetic starting at 4.00 pm and he was discharged the following morning.
This is the ultrasound scan I took 30 hours after the operation. A central cavity is seen, similar to those seen after open prostatectomy.

I would appreciate comments from visitors to this blog.
Friday, February 03, 2006
Videos in this blog
I have just found out a way to include videos in this blog. This gives me the chance to show videos that can be useful for patients as well as to share my experience and tips and tricks with other doctors interested in PVP - Photoselective vaporization of the prostate. This video shows a PVP performed on a patient with Benign Prostatic Hyperplasia (BPH) with very bothersome symptoms and a 44 gram prostate. The procedure took about an hour, I kept a catheter in for six hours and I took it out leaving 250 cc of saline inside the bladder. The patient voided wonderfully and was discharged the same day, eight ours after finishing the operation.... check it out.
Subscribe to:
Posts (Atom)

