

Urologist · HoLEP Specialist · Robotic Surgeon · ICUA Madrid
 He had a long urethral stenosis involving bulbar and penile urethra, and when we explored it surgically it affected all the length of the urethra. The operation was uneventful and we needed 4 hours to reconstruct it with a combination of free grafts taken from the inner side of the cheek (Barbagli's operation) and a long cutaneous flap from the penis (Orandi's operation). I was told that all the patients we have operated up to now are doing well. I am happy for them.
He had a long urethral stenosis involving bulbar and penile urethra, and when we explored it surgically it affected all the length of the urethra. The operation was uneventful and we needed 4 hours to reconstruct it with a combination of free grafts taken from the inner side of the cheek (Barbagli's operation) and a long cutaneous flap from the penis (Orandi's operation). I was told that all the patients we have operated up to now are doing well. I am happy for them.

 In this ocassion, we had 16 students who had the opportunity of attending comprehensive conferences on renal laparoscopy, sessions of full time surgical videos analysis and to experimental surgical theatres. There were six invited professors including me and we had the privilege of having Dr. Hervé Baumert with us. He is currently working in Paris and Cambridge and is considered one of the top laparoscopic urologists in the world. We were amazed by his impressive collection of surgical videos.
In this ocassion, we had 16 students who had the opportunity of attending comprehensive conferences on renal laparoscopy, sessions of full time surgical videos analysis and to experimental surgical theatres. There were six invited professors including me and we had the privilege of having Dr. Hervé Baumert with us. He is currently working in Paris and Cambridge and is considered one of the top laparoscopic urologists in the world. We were amazed by his impressive collection of surgical videos.
 . This way, students had access to theoretical knowledge on advanced renal laparoscopy, and also to the experimental surgical theatre, where they could train on the different surgical operations performed on kidney and ureter (radical nephrectomy, partial nephrectomy, and so on and so forth), while they were able to experience the newest surgical instruments and devices, as the new Harmonic dissection device from Ethicon, and other useful devices in renal surgery, as the LapraTy, Hemolock, etc..
. This way, students had access to theoretical knowledge on advanced renal laparoscopy, and also to the experimental surgical theatre, where they could train on the different surgical operations performed on kidney and ureter (radical nephrectomy, partial nephrectomy, and so on and so forth), while they were able to experience the newest surgical instruments and devices, as the new Harmonic dissection device from Ethicon, and other useful devices in renal surgery, as the LapraTy, Hemolock, etc..
 Today I took a plane with my colleague, Dr. Castillón to participate in a training session on Robotic Radical Prostatectomy with the Da Vinci system. This system allows the surgeon to operate from a surgical station, as in the photograph, and provides 3D visualization of the operative field inside the abdomen. This is the state of the art treatment for localised prostate cancer and it allows to obtain spectacular oncological results, as well as high rates of urinary continence and sexual potency preservation after this operation, that are not obtainable with open surgery.
Today I took a plane with my colleague, Dr. Castillón to participate in a training session on Robotic Radical Prostatectomy with the Da Vinci system. This system allows the surgeon to operate from a surgical station, as in the photograph, and provides 3D visualization of the operative field inside the abdomen. This is the state of the art treatment for localised prostate cancer and it allows to obtain spectacular oncological results, as well as high rates of urinary continence and sexual potency preservation after this operation, that are not obtainable with open surgery.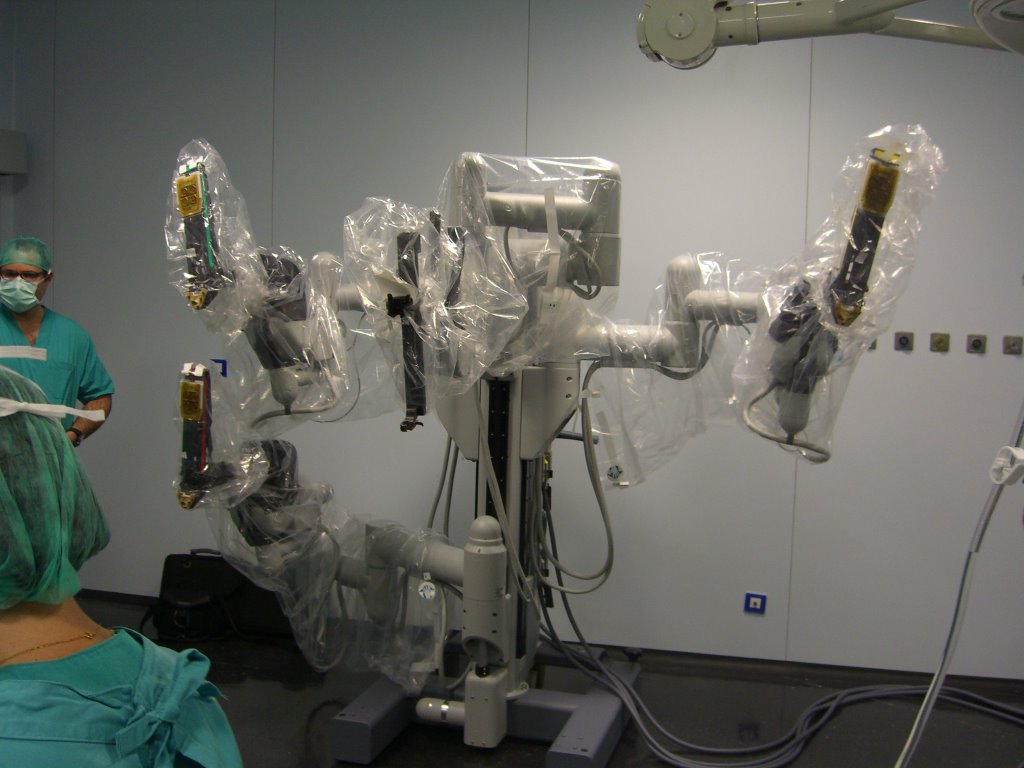 This is the robot and the four arms, it will be position by the patient and the robot will manipulate the surgical instruments. It is a slave robot, it obeys the movements of the surgeon hands, that holds two very sophisticated Joysticks with his hands. The robot even corrects tremor of the surgeon's hands. 3D vision inside the abdomen helps visualizing tissues with unseen quality of image and enhancement.
This is the robot and the four arms, it will be position by the patient and the robot will manipulate the surgical instruments. It is a slave robot, it obeys the movements of the surgeon hands, that holds two very sophisticated Joysticks with his hands. The robot even corrects tremor of the surgeon's hands. 3D vision inside the abdomen helps visualizing tissues with unseen quality of image and enhancement. The surgeon is relaxed, sitting in the surgical console, and an assistant changes the instruments of the robot when the surgeon requests it. It is no doubt the way surgery will follow in the future.
The surgeon is relaxed, sitting in the surgical console, and an assistant changes the instruments of the robot when the surgeon requests it. It is no doubt the way surgery will follow in the future. Once again I flew to La Coruña to participate in a training session. In this ocassion we had a difficult case, a patient with a 135 gram prostate. After spending the afternoon there, I took the plane back to Madrid. This is a busy week, this Thursday I will do an early morning PVP and then I will take the plane to Bilbao, in the north of Spain. I am going to witness a case of radical
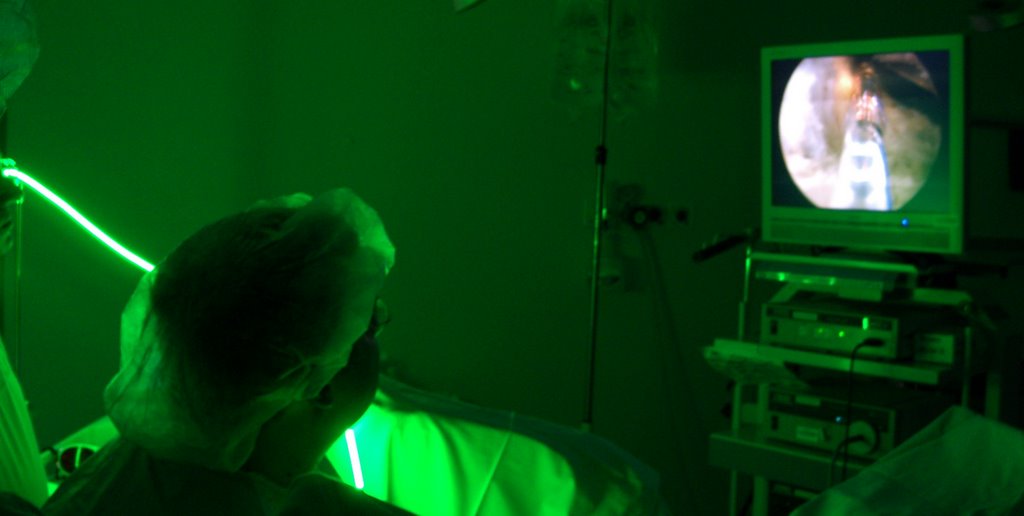
Once again I flew to La Coruña to participate in a training session. In this ocassion we had a difficult case, a patient with a 135 gram prostate. After spending the afternoon there, I took the plane back to Madrid. This is a busy week, this Thursday I will do an early morning PVP and then I will take the plane to Bilbao, in the north of Spain. I am going to witness a case of radical The black piece is the telescope's visor, traditionally one would look through it with the naked eye, but when working with lasers eye protection is a must, that is why we connect this visor to a surgical endoscopic video camera, but in order to protect the camera from the intensity of the greenlight laser (the reflection of the laser light could break the camera), we use a filter between the visor and the camera. This explains why in the photographs of the technique I publish here, the laser fibre appears green, but in the endoscopic videos the laser light looks like orange. This filter blocks the specific wavelenght of the greenlight laser (532 nm).
The black piece is the telescope's visor, traditionally one would look through it with the naked eye, but when working with lasers eye protection is a must, that is why we connect this visor to a surgical endoscopic video camera, but in order to protect the camera from the intensity of the greenlight laser (the reflection of the laser light could break the camera), we use a filter between the visor and the camera. This explains why in the photographs of the technique I publish here, the laser fibre appears green, but in the endoscopic videos the laser light looks like orange. This filter blocks the specific wavelenght of the greenlight laser (532 nm).
 Yesterday I received confirmation of an invitation to travel to South Africa to participate in lectures in different cities on Greenlight PVP (Photoselective Vaporization of the Prostate).
Yesterday I received confirmation of an invitation to travel to South Africa to participate in lectures in different cities on Greenlight PVP (Photoselective Vaporization of the Prostate).
 Today I have participated in the Urology International Congress celebrated at the Hospital Miguel Servet, from Zaragoza, organised by profs. Rioja, Liédana y Roncales. It is a very impressive congress, the organization was superb and the scientific program very attractive. Multiple national and international experts were invited. The conference hall had three giant screens where urologists attending the congress could see three simultaneous surgical interventions and hear one of the three conversations going on between the surgeons and the moderators of each surgical session. Congratulations to the organisers!!!.
Today I have participated in the Urology International Congress celebrated at the Hospital Miguel Servet, from Zaragoza, organised by profs. Rioja, Liédana y Roncales. It is a very impressive congress, the organization was superb and the scientific program very attractive. Multiple national and international experts were invited. The conference hall had three giant screens where urologists attending the congress could see three simultaneous surgical interventions and hear one of the three conversations going on between the surgeons and the moderators of each surgical session. Congratulations to the organisers!!!.
 This Hospital Miguel Servet is interestingly in front of the football stadium "La Rosaleda", where the local team scored 6 goals to Real Madrid football club, who could one produce one miserable goal. I have had the strange feeling that everybody here looked suspiciously happy and their smiles were probably wider than usual. I am not exactly a football fan, but one perceives these things..... and my team is Real Madrid.
This Hospital Miguel Servet is interestingly in front of the football stadium "La Rosaleda", where the local team scored 6 goals to Real Madrid football club, who could one produce one miserable goal. I have had the strange feeling that everybody here looked suspiciously happy and their smiles were probably wider than usual. I am not exactly a football fan, but one perceives these things..... and my team is Real Madrid. Then it was my turn. The PVP operation was uneventful and I was able to vaporise BPH tissue and reach the capsule of the prostate in just 45 minutes. During the operation, I had a microphone that allowed me to explain the operation and I also had an interesting conversation with the moderator, Dr. Miñana, who posed very interesting questions. I tried to summarize the advantages of this technique as well as the mechanisms of laser and tissue interactions. The audience was very impressed, specially after having seen a monopolar resection, which did not avoid bleeding.
Then it was my turn. The PVP operation was uneventful and I was able to vaporise BPH tissue and reach the capsule of the prostate in just 45 minutes. During the operation, I had a microphone that allowed me to explain the operation and I also had an interesting conversation with the moderator, Dr. Miñana, who posed very interesting questions. I tried to summarize the advantages of this technique as well as the mechanisms of laser and tissue interactions. The audience was very impressed, specially after having seen a monopolar resection, which did not avoid bleeding. Today I travelled to Barcelona to participate in a training session on PVP (Photoselective Vaporization of the Prostate) for BPH (Benign Prostatic Hyperplasia). We did two cases, one was a very high risk patient, who was obese, and had an aortic aneurism, dilated myocardiopathy and other serious conditions. His prostate was relatively big, with 90 grams. The operation was uneventful and today we managed to finally operate him, as this time he did not take biscuits just before scheduled surgery (some days ago we had to cancel the operation for this reason). In spite of the high surgical risk, we managed to operate him and to let him catheter-free. He had been catheterised due to an acute retention of urine and after that, he was unable to void spontaneously. Then we did an easier case, a 60 g prostate, that was also uneventful. I then took a car and drove towards Zaragoza, a three hour trip to reach this city. Tomorrow I have to participate in the International Congress performing a live PVP in front of 200 + urologists from Spain and other countries.
Today I travelled to Barcelona to participate in a training session on PVP (Photoselective Vaporization of the Prostate) for BPH (Benign Prostatic Hyperplasia). We did two cases, one was a very high risk patient, who was obese, and had an aortic aneurism, dilated myocardiopathy and other serious conditions. His prostate was relatively big, with 90 grams. The operation was uneventful and today we managed to finally operate him, as this time he did not take biscuits just before scheduled surgery (some days ago we had to cancel the operation for this reason). In spite of the high surgical risk, we managed to operate him and to let him catheter-free. He had been catheterised due to an acute retention of urine and after that, he was unable to void spontaneously. Then we did an easier case, a 60 g prostate, that was also uneventful. I then took a car and drove towards Zaragoza, a three hour trip to reach this city. Tomorrow I have to participate in the International Congress performing a live PVP in front of 200 + urologists from Spain and other countries.

 Today I took a flight to Barcelona to participate in a training session on PVP - Photoselective vaporization of the prostate. We had programmed two patients, the first case was straightforward, the second was very complex. The second patient in the list had morbid obesity and respiratory problems, and we planned to operate him in the sitting position, to increase the chances for him to tolerate the operation. His prostate was relatively big, weighing 100 g. The first case was uneventful, the second case was cancelled because the patient did not respect the "nil per mouth" instruction and he had had breakfast consisting in coffee and cookies. The anaesthesiologist thought we could not operate him with a full stomach, so we have rescheduled him for another date and I went back to Madrid.
Today I took a flight to Barcelona to participate in a training session on PVP - Photoselective vaporization of the prostate. We had programmed two patients, the first case was straightforward, the second was very complex. The second patient in the list had morbid obesity and respiratory problems, and we planned to operate him in the sitting position, to increase the chances for him to tolerate the operation. His prostate was relatively big, weighing 100 g. The first case was uneventful, the second case was cancelled because the patient did not respect the "nil per mouth" instruction and he had had breakfast consisting in coffee and cookies. The anaesthesiologist thought we could not operate him with a full stomach, so we have rescheduled him for another date and I went back to Madrid.
 Today, a saturday, I took an early plane to Valencia in order to participate in a training session on KTP laser for the treatment of Benign Prostatic Hyperplasia. I operated a high risk patient with a 100 gram prostate. The operation was uneventful and I hope the patient will go home later today.
Today, a saturday, I took an early plane to Valencia in order to participate in a training session on KTP laser for the treatment of Benign Prostatic Hyperplasia. I operated a high risk patient with a 100 gram prostate. The operation was uneventful and I hope the patient will go home later today.
 Today we have used for the first time our new Holmium laser, Stonelight, manufactured by Laserscope.
Today we have used for the first time our new Holmium laser, Stonelight, manufactured by Laserscope.


 Our institution, the Institute of Advanced Urological Surgery, has reached an agreement with Dr. Gastón to bring him over to Madrid to operate our patients so they can have access to a world leader in prostate cancer surgery without having to leave their country.
Our institution, the Institute of Advanced Urological Surgery, has reached an agreement with Dr. Gastón to bring him over to Madrid to operate our patients so they can have access to a world leader in prostate cancer surgery without having to leave their country.
 Today I have received a copy of the fourth volume of the Audiovisual Course on New Technologies in Urology. A training programme sponsored by Pfizer and supported by the Spanish Urological Association. I already contributed for volume I with a video and a chapter on PVP - Photoselective Vaporization of the Prostate. In this volume IV I have published an article and a video on Cryosurgical ablation of prostate cancer. This is an interesting video, it includes images of the 4D transrectal ultrasound monitorization of the procedure, a new approach we performed at the Instituto de Cirugía Urológica Avanzada (ICUA), in Madrid.
Today I have received a copy of the fourth volume of the Audiovisual Course on New Technologies in Urology. A training programme sponsored by Pfizer and supported by the Spanish Urological Association. I already contributed for volume I with a video and a chapter on PVP - Photoselective Vaporization of the Prostate. In this volume IV I have published an article and a video on Cryosurgical ablation of prostate cancer. This is an interesting video, it includes images of the 4D transrectal ultrasound monitorization of the procedure, a new approach we performed at the Instituto de Cirugía Urológica Avanzada (ICUA), in Madrid.
 This Monday, December 19th, I went to La Coruña again to participate in a Photoselective vaporization of the prostate (PVP) surgical training session. We did two operations, the morning session on a patient with a 70 gram prostate and the afternoon session on a patient with a 90 gram prostate. The day was uneventful, we had time to go a wonderful restaurant for lunch, with a view of La Coruña. Octopus is the local specialty and it is delicious. I then came back to Madrid, the following day I had to operate a friend who is a Doctor and his prostate volume was 105 cc. The operation was also uneventful and I was able to discharge him in the afternoon, after two and a half hours of PVP. The more PVPs I do, the more I like PVP, recovery is so spectacular, patients go back to their normal lifes, and results are so good!!!
This Monday, December 19th, I went to La Coruña again to participate in a Photoselective vaporization of the prostate (PVP) surgical training session. We did two operations, the morning session on a patient with a 70 gram prostate and the afternoon session on a patient with a 90 gram prostate. The day was uneventful, we had time to go a wonderful restaurant for lunch, with a view of La Coruña. Octopus is the local specialty and it is delicious. I then came back to Madrid, the following day I had to operate a friend who is a Doctor and his prostate volume was 105 cc. The operation was also uneventful and I was able to discharge him in the afternoon, after two and a half hours of PVP. The more PVPs I do, the more I like PVP, recovery is so spectacular, patients go back to their normal lifes, and results are so good!!!

Dr. Fernando Gómez Sancha
Urologist. HoLEP and robotic surgery specialist. Head of Urology at Clínica CEMTRO, Madrid. I have operated in over 50 countries and performed more than 10,000 laser procedures.
