
 We took a morning flight to Cape Town. The most turistic city of South Africa. One could say Cape Town is like Marbella in Spain. The Weather was splendid, but we did not have much time to visit the city. Just after arriving to Cape Town, we went to the University Hospital, where the urology staff attended my lecture, that was followed by an animated discussion.
We took a morning flight to Cape Town. The most turistic city of South Africa. One could say Cape Town is like Marbella in Spain. The Weather was splendid, but we did not have much time to visit the city. Just after arriving to Cape Town, we went to the University Hospital, where the urology staff attended my lecture, that was followed by an animated discussion.  It seems that public hospitals will take some time before adopting this technique, mainly because of lack of funds to invest in new technologies. One of the questions asked by these urologists was that with PVP there is no tissue that can be sent to the pathologist for histological analysis. I explained that if a tumor is suspected, then biopsies are indicated prior to PVP. Also I told them that when we decide to treat a patient with drugs, there is no tissue for histology...
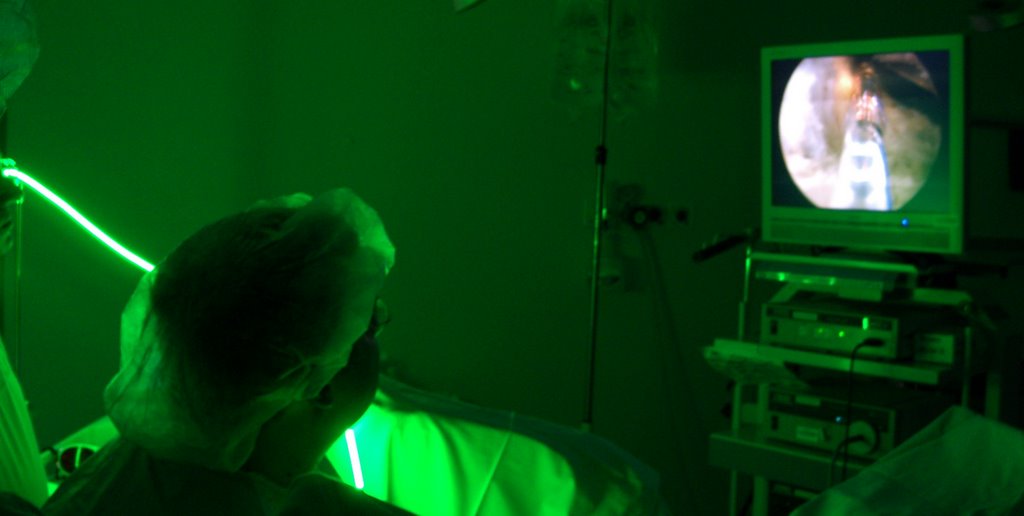
It seems that public hospitals will take some time before adopting this technique, mainly because of lack of funds to invest in new technologies. One of the questions asked by these urologists was that with PVP there is no tissue that can be sent to the pathologist for histological analysis. I explained that if a tumor is suspected, then biopsies are indicated prior to PVP. Also I told them that when we decide to treat a patient with drugs, there is no tissue for histology...
Then we rushed out of there because at 6.30 pm we had another lecture where all urologists in private practice in the city were invited.
 Again I observed the same effect in the urologists attending this lecture, they were fascinated by PVP. When we were finishing the lecture we started hearing explosions outside, and when we went out to find out, a fantastic fireworks show had started. A good end for this lecture.... Tomorrow we will travel to Durban, to participate in the last lecture scheduled in this hectic roadshow.
Again I observed the same effect in the urologists attending this lecture, they were fascinated by PVP. When we were finishing the lecture we started hearing explosions outside, and when we went out to find out, a fantastic fireworks show had started. A good end for this lecture.... Tomorrow we will travel to Durban, to participate in the last lecture scheduled in this hectic roadshow. 







 Then we travelled to Pretoria where the first lecture should take place.
Then we travelled to Pretoria where the first lecture should take place.



























{kind=link}